Pain can be very confusing. One of my most important jobs is to answer the question “What is causing my pain?”. This may seem straightforward but it is very common that the site of pain is not actually the cause of pain. Sciatica and “pinched nerves” help illustrate this concept. To better answer the question “What is causing my pain?” I want to highlight the difference between referred pain and radicular pain. Both types of pain result in the source of the pain and the site of pain being different. Once we better understand the difference between referred and radicular pain we can dive into sciatica.
Some common conditions treated at OMNE Chiropractic that result in pain that travels or spreads.
- Sciatica
- Piriformis syndrome
- Radiculopathy
- Disc herniations/bulges
- “Pinched nerves”
- Pseudo-sciatica
- Peripheral Nerve Entrapments
- Carpal Tunnel Syndrome
- Cubital Tunnel Syndrome
Sciatica: Getting the right diagnosis
Failure to distinguish the difference between referred and radicular pain leads to mismanagement resulting in increased suffering and cost. Our Omaha chiropractic office spends more time with assessment of our patients so we can be sure we get the diagnosis correct and treatment can be focused and effective. This saves patients time, money, and suffering.

Referred Pain
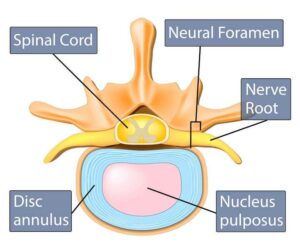
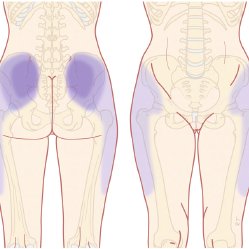
Referred pain occurs when pain producing structures of the spine spread into the extremities. In this case, the pain producing structures of the spine are discs, facet joints, muscles, and sacroiliac joints. The quality of referred pain is generally described as dull, achy, and pressure. One of the hallmark features is that the boundaries may be difficult to define but the core can be confidently located. However, once the area of pain is established it tends to be fixed in location.
X-rays, MRIs, and CT scans are not indicated or particularly useful in distinguishing the cause of referred pain. Taking fancy pictures using advanced imaging of referred pain is likely to lead to a high false positive rate that will likely lead to mismanagement including unnecessary and harmful injections, medications, and surgeries.
Radicular Pain
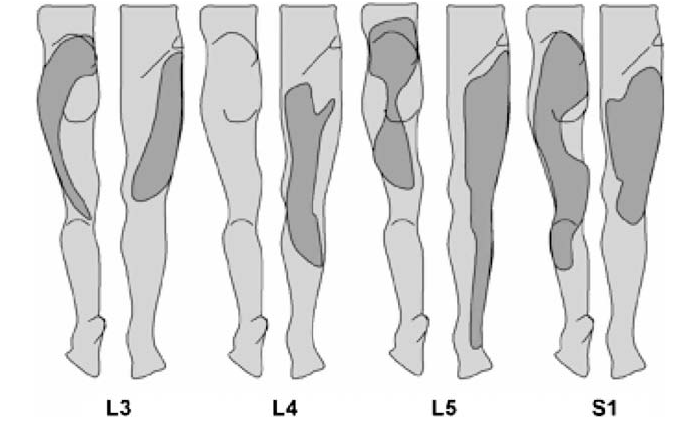
On the contrary, radicular pain is over-diagnosed and often mismanaged. For pain to be truly radicular it must be the result of symptoms from the nerve root – a specific portion of the nerve in the spinal column. The most common cause of radicular pain are disc herniations when the disc becomes damaged it releases inflammatory mediators that irritate the nerve root. Radicular pain is distinct in that is travels along the length of the lower limb in a distribution that is between 2-3 inches wide.
Guess how they found out the clinical features of radicular pain – awake patients had surgery for disc herniations and they squeezed their nerves with forceps….no thank you.
Back pain and referred pain are common, true radicular pain is not. When radicular pain is being strictly defined, its prevalence is only about 12% or less (Bogduk N. (2009))
What is sciatica; referred or radicular?
The problem with sciatica is that it means different things to different people, making it a somewhat poor diagnosis.
In a perfect world, the diagnosis is one or the other. Unfortunately, it is quite a bit more complex than that as referred and radicular pain is not mutually exclusive and often co-exist. Let me explain.
A common scenario is a patient presents with back, hip, and leg pain. Without any testing and strictly off the area of the pain this could be both radicular and/or referred pain. This type of pain distribution is common in our Omaha chiropractic office. The pain in the back may be related to a disc herniation and is localized to the lower back. Eventually, the disc sustains additional injury and inflammation begins to irritate the nearby nerve root resulting in radicular pain. Perhaps the radicular pain requires additional intervention outside our chiropractic office. A referral is placed to get a lumbar epidural steroid injection or oral steroid. This helps the radicular pain, but the patient continues to have back pain that is being simultaneously treated in our office. This is one reason why we continue to see patients that have undergone epidurals.
The complex nature of referred and radicular pain is why many exercises found on the internet are not successful in treating back and leg pain. Dr. Peters is passionate about correctly categorizing the pain and finding solutions. Schedule an appointment with our Omaha chiropractic office if you are looking for solutions to back pain, leg pain, or sciatica.